Coronary Artery Disease (CAD): Causes, Symptoms & Treatment
Coronary artery disease is the build-up of plaque in the arteries that feed the heart — the leading cause of heart attacks. Here's how it develops, how it's found, and how it's treated.
What is coronary artery disease?
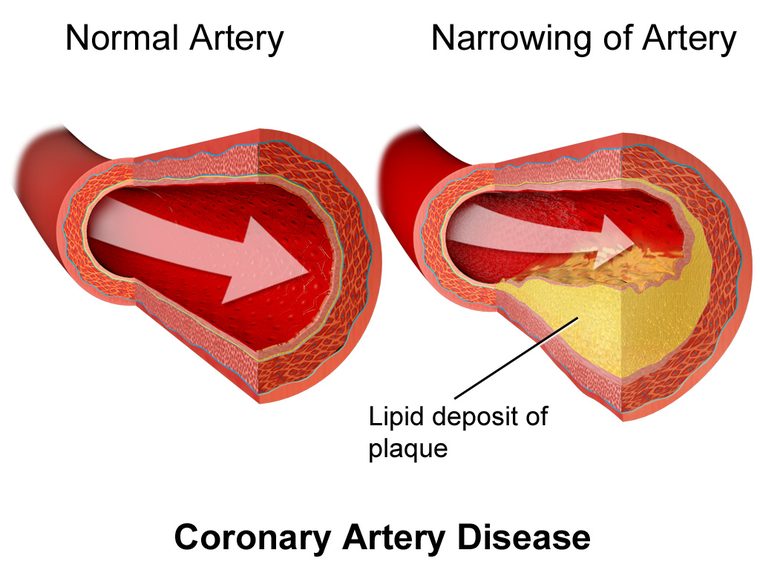
Coronary artery disease (CAD) — also called coronary heart disease or ischaemic heart disease — is the narrowing of the coronary arteries by atherosclerosis, a slow build-up of cholesterol-laden plaque in the artery wall. The coronary arteries are the heart's own fuel lines; when they narrow, the heart muscle can't get the oxygen it needs, especially under stress. CAD is the leading cause of death worldwide, and it is the reason most people end up in a cardiac cath lab.
How atherosclerosis develops
Atherosclerosis begins quietly, often decades before symptoms. Cholesterol — particularly LDL ("bad") cholesterol — infiltrates the artery lining, triggering inflammation. Immune cells engulf the cholesterol to form foam cells, and over years a plaque grows, made of a fatty core under a fibrous cap.
Plaque causes trouble two ways. A large, stable plaque gradually narrows the lumen and limits flow, producing predictable exertional angina. A vulnerable plaque with a thin cap can suddenly rupture; the body treats the exposed core like an injury and forms a clot on top, which can abruptly block the artery and cause a heart attack. This is why the "size" of a narrowing doesn't fully predict risk — plaque stability matters as much as severity.

Risk factors
CAD is largely a disease of accumulated risk. The good news is that most of the drivers can be changed.
| Modifiable | Non-modifiable |
|---|---|
| Smoking | Increasing age |
| High LDL cholesterol | Male sex (women catch up after menopause) |
| High blood pressure | Family history of premature CAD |
| Diabetes | Genetics / ethnicity |
| Obesity, inactivity, poor diet |
Because these factors compound, clinicians estimate an individual's overall risk to decide how aggressively to treat — for example, when to start a statin. Controlling the modifiable factors is the foundation of both prevention and treatment.
Symptoms
The hallmark of CAD is angina — a pressure, tightness, or squeezing in the chest, often radiating to the arm, jaw, or back, brought on by exertion or stress and relieved within minutes by rest or nitroglycerin. This predictable, effort-related pattern is stable angina.
A change in that pattern — angina at rest, or that is new, more frequent, or more severe — is unstable angina, part of the acute coronary syndrome spectrum and a warning of an unstable plaque. Other symptoms include breathlessness, fatigue, and reduced exercise tolerance. Importantly, presentations are frequently atypical in women, older adults, and people with diabetes, who may have only fatigue, indigestion-like discomfort, or breathlessness — a major reason CAD is underdiagnosed in these groups. Some people have no symptoms at all until a heart attack.
How CAD is diagnosed
Diagnosis combines the clinical picture with testing that ranges from non-invasive to invasive:
- ECG — may show ischaemic ST-T changes or evidence of a prior infarction; often normal at rest.
- Stress testing — exercise or pharmacologic, with ECG, nuclear perfusion, or stress echo, to unmask ischaemia.
- CT coronary angiography and calcium scoring — increasingly used non-invasive imaging that can rule out significant disease.
- Invasive coronary angiography — the definitive test, directly visualising the arteries, often with FFR or intravascular imaging (IVUS/OCT) to judge whether a narrowing is truly flow-limiting.
- Blood tests — a lipid profile, glucose/HbA1c, and, in acute presentations, troponin.
Treatment
Treating CAD has two goals: relieve symptoms and prevent heart attacks and death. It rests on three pillars.
| Pillar | Details |
|---|---|
| Lifestyle | Stop smoking, a heart-healthy diet, regular exercise, and weight control — the highest-value interventions. |
| Medications | Statins (and other lipid-lowering drugs) to stabilise plaque and lower LDL; antiplatelets such as aspirin; blood-pressure control; and anti-anginals (beta-blockers, nitrates, calcium channel blockers). |
| Revascularisation | PCI with stenting for suitable lesions, or coronary artery bypass grafting (CABG) for complex or multivessel disease. |
For stable CAD, medications and lifestyle ("optimal medical therapy") are the foundation, with revascularisation added for ongoing symptoms or high-risk anatomy. In an acute coronary syndrome, the priority shifts to urgent restoration of blood flow — emergency PCI for a STEMI, guided by the culprit artery.
Living with CAD & prognosis
CAD is a chronic condition, but it is highly modifiable. Consistent risk-factor control — not smoking, keeping LDL low, managing blood pressure and diabetes, and staying active — dramatically lowers the chance of a future heart attack, and cardiac rehabilitation improves outcomes after an event. Many people live full, active lives with well-managed coronary disease.
Key takeaways
- CAD is atherosclerotic narrowing of the coronary arteries — the leading cause of death worldwide.
- Plaque can slowly limit flow (stable angina) or rupture and clot (heart attack).
- Risk factors are largely modifiable — smoking, cholesterol, blood pressure, diabetes.
- Diagnosis spans ECG, stress testing, CT, and invasive angiography with FFR.
- Treatment = lifestyle + medications (statins, antiplatelets) + revascularisation (PCI/CABG).
Learn how CAD is treated in the lab
Understand PCI, stenting, and cardiac catheterization.
PCI vs Cardiac Cath →Frequently asked questions
What is coronary artery disease?
The narrowing of the coronary arteries by atherosclerotic plaque, which limits blood flow to the heart muscle and can cause angina or a heart attack. It is the leading cause of death worldwide.
What causes coronary artery disease?
Atherosclerosis — a build-up of cholesterol plaque driven by high LDL cholesterol, smoking, high blood pressure, diabetes, obesity, inactivity, and genetic risk.
What are the symptoms of coronary artery disease?
Angina (exertional chest pressure relieved by rest or nitroglycerin), breathlessness, and fatigue; symptoms are often atypical in women, older adults, and people with diabetes, and some are asymptomatic until a heart attack.
What is the difference between stable and unstable angina?
Stable angina is predictable, effort-related chest pain relieved by rest; unstable angina is new, worsening, or rest pain that signals an unstable plaque and is a medical emergency.
How is coronary artery disease diagnosed?
With an ECG, stress testing, CT coronary angiography or calcium scoring, and invasive coronary angiography — sometimes with FFR or intravascular imaging — plus blood tests.
How is coronary artery disease treated?
Lifestyle changes, medications (statins, antiplatelets, blood-pressure and anti-anginal drugs), and revascularisation with PCI (stenting) or bypass surgery when needed.
Can coronary artery disease be reversed?
Progression can be halted and plaque stabilised with aggressive risk-factor control and statins; while established plaque rarely disappears, the risk of a heart attack falls substantially.
Sources & further reading
- Cardiovascular Credentialing International (CCI)
- American College of Cardiology
- American Heart Association
- MedlinePlus (U.S. National Library of Medicine)
External links are provided for reference; always confirm current details with the official source.