Atrial Fibrillation (AFib): ECG, Risks & Treatment
Atrial fibrillation is the most common sustained arrhythmia — a fast, disorganised atrial rhythm that raises the risk of stroke. Here's how it looks on the ECG, why it matters, and how it's treated.
- What is atrial fibrillation?
- Atrial fibrillation on the ECG
- Why atrial fibrillation happens
- Types of atrial fibrillation
- Causes and risk factors
- Symptoms
- Why AFib matters: stroke and heart failure
- How atrial fibrillation is diagnosed
- Estimating stroke risk: CHA₂DS₂-VASc
- Blood thinners: preventing stroke
- Controlling the heartbeat: rate vs rhythm
- Catheter ablation
- Lifestyle and risk-factor modification
- Key takeaways
What is atrial fibrillation?
Atrial fibrillation (AFib or AF) is the most common sustained heart-rhythm disorder — a state in which the upper chambers of the heart, the atria, are driven by rapid, chaotic electrical signals so they quiver instead of contracting in a coordinated way. Instead of the single, organised impulse of a normal heartbeat, hundreds of disorganised electrical wavelets swirl through the atria, bombarding the AV node. The AV node lets only some of them through, at random, which is why the pulse in atrial fibrillation is classically irregularly irregular — with no pattern at all to the timing of the beats.
Because the atria no longer contract effectively, they lose the "atrial kick" that normally tops up the ventricles at the end of filling — costing up to a fifth of the heart's output. More importantly, blood that isn't pushed out briskly can stagnate and clot, which is the root of atrial fibrillation's most feared complication: stroke. AFib affects tens of millions of people worldwide, becomes far more common with age, and is a frequent finding for anyone working in cardiovascular care.
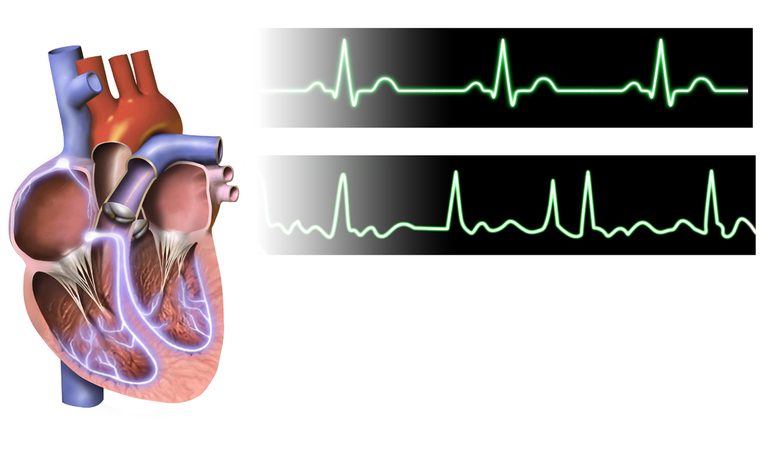
Atrial fibrillation on the ECG
The ECG is how atrial fibrillation is diagnosed, and it has three unmistakable features. Learn to recognise them and you'll spot AFib in seconds.

- Irregularly irregular R–R intervals. The spacing between beats is random — this is the single most reliable sign.
- No discernible P waves. The organised atrial depolarisation is gone, replaced by a wavering fibrillatory (f-wave) baseline.
- A narrow QRS in most cases, because the ventricles are still activated through the normal conduction system.
The ventricular rate can be fast ("AFib with rapid ventricular response," often 110–170 bpm) or well controlled. Sharpen your eye on our rhythm interpretation guide and compare it against a normal ECG.
Why atrial fibrillation happens
Atrial fibrillation usually begins with rapidly firing triggers, most often located where the pulmonary veins join the left atrium. Once these triggers set the atria fibrillating, the arrhythmia sustains itself through re-entry — self-perpetuating electrical circuits in atrial tissue that has become electrically and structurally abnormal.
Crucially, AFib tends to beget more AFib. The longer the atria fibrillate, the more they remodel — the tissue changes in ways that make the arrhythmia easier to trigger and harder to stop. This is why modern guidelines increasingly favour treating atrial fibrillation early, before extensive remodelling sets in, and why they frame AFib as a progressive disease rather than a one-off event.
Types of atrial fibrillation
Atrial fibrillation is classified by how it behaves over time, which shapes the treatment approach:
| Type | Definition |
|---|---|
| Paroxysmal | Comes and goes, terminating on its own (or within 7 days) |
| Persistent | Lasts longer than 7 days and needs cardioversion or drugs to stop |
| Long-standing persistent | Continuous for more than a year but rhythm control is still being pursued |
| Permanent | Accepted as ongoing; rhythm control is no longer attempted |
Recent guidelines also describe AFib as a continuum of stages — from being at risk, through pre-clinical and clinical AFib, to permanent — reflecting that it is a progressive condition best managed proactively.
Causes and risk factors
Many conditions promote the atrial stretch and scarring that set the stage for AFib. Recognising them matters, because several are modifiable — and treating them is now considered a core pillar of AFib care.
- Age — the single biggest risk factor; prevalence rises steeply after 65.
- High blood pressure — the most common modifiable driver.
- Obesity, physical inactivity, and obstructive sleep apnea — increasingly recognised as major, reversible contributors.
- Alcohol — even moderate intake raises risk; a binge can trigger acute AFib ("holiday heart syndrome").
- Heart disease — valve disease (especially mitral), heart failure, prior heart attack, and cardiomyopathy.
- Hyperthyroidism, diabetes, chronic kidney disease, and pulmonary disease.
- Acute stressors — infection, surgery (especially cardiac), and electrolyte disturbance.
Symptoms
Atrial fibrillation is remarkably variable. Some people are severely limited; others feel nothing at all and are diagnosed only when AFib is found incidentally — or, tragically, when it first announces itself as a stroke. Typical symptoms include:
- Palpitations — a racing, fluttering, or pounding heartbeat
- Breathlessness and reduced exercise tolerance
- Fatigue, light-headedness, or dizziness
- Chest discomfort, and occasionally fainting
Because "silent" AFib carries the same stroke risk as symptomatic AFib, screening — including with modern smartwatches and single-lead recorders — has become an important way to catch it.
Why AFib matters: stroke and heart failure
The reason atrial fibrillation commands so much attention is its complications.

- Stroke. A poorly contracting left atrium — especially the pouch-like left atrial appendage — lets blood stagnate and clot. If a clot breaks off, it can travel to the brain. AFib raises stroke risk roughly fivefold, and AFib-related strokes tend to be more severe.
- Heart failure. A persistently fast, irregular rhythm can weaken the heart over time (tachycardia-induced cardiomyopathy), and AFib and heart failure often worsen each other.
- Reduced quality of life and a modestly higher risk of cognitive decline.
How atrial fibrillation is diagnosed
A standard 12-lead ECG confirms AFib when it's present during the recording. Because paroxysmal AFib comes and goes, catching it can take longer monitoring:
- Holter monitor — continuous recording over 24–48 hours or longer.
- Event or patch monitors — worn for days to weeks to capture intermittent episodes.
- Implantable loop recorders — for very infrequent episodes or after a stroke of unknown cause.
- Consumer devices — smartwatches and single-lead recorders increasingly flag possible AFib, which is then confirmed on a formal ECG.
An echocardiogram is usually done to assess the heart's structure, valves, and function.
Estimating stroke risk: CHA₂DS₂-VASc
Not everyone with AFib needs a blood thinner — the decision hinges on their stroke risk, estimated with the CHA₂DS₂-VASc score:
| Factor | Points |
|---|---|
| C — Congestive heart failure / LV dysfunction | 1 |
| H — Hypertension | 1 |
| A₂ — Age ≥ 75 | 2 |
| D — Diabetes | 1 |
| S₂ — Prior Stroke / TIA / thromboembolism | 2 |
| V — Vascular disease | 1 |
| A — Age 65–74 | 1 |
| Sc — Sex category (female) | 1 |
In general, a score of 2 or more in men (3 or more in women) means anticoagulation is recommended; a score of 0 (men) or 1 (women) is low-risk. Bleeding risk is weighed too — often with the HAS-BLED score — but a high bleeding score is a prompt to fix reversible risks, not usually a reason to withhold protection.
Blood thinners: preventing stroke
Anticoagulation ("blood thinners") is the cornerstone of AFib management, and it's what people most often search for. Two options dominate:
| DOACs | Warfarin | |
|---|---|---|
| Examples | Apixaban, rivaroxaban, dabigatran, edoxaban | Warfarin |
| Monitoring | None routine | Regular INR blood tests |
| Diet/drug interactions | Fewer | Many |
| Preferred? | First-line for most | Mechanical valves, moderate–severe mitral stenosis |
Direct oral anticoagulants (DOACs) are now recommended over warfarin for most people with AFib, because they are at least as effective at preventing stroke, cause less brain bleeding, and don't need INR monitoring. Antiplatelet drugs like aspirin are not adequate substitutes for stroke prevention in AFib.
For patients who genuinely cannot take long-term anticoagulation (for example, recurrent serious bleeding), left atrial appendage occlusion — a device such as the Watchman that seals off the appendage where most clots form — is an alternative. Explore the drug classes in our cath-lab medications guide.
Controlling the heartbeat: rate vs rhythm
Alongside stroke prevention, treatment targets the rhythm itself, in one of two strategies (often combined):
| Strategy | Goal | How |
|---|---|---|
| Rate control | Slow the ventricular response, leaving AFib in place | Beta-blockers, non-dihydropyridine calcium channel blockers (diltiazem, verapamil), sometimes digoxin |
| Rhythm control | Restore and maintain normal sinus rhythm | Antiarrhythmic drugs, electrical or chemical cardioversion, and catheter ablation |
Cardioversion — a synchronised electrical shock or an antiarrhythmic drug — can reset the rhythm. Because restoring sinus rhythm can dislodge a clot, patients must be adequately anticoagulated (or have a clot excluded on transoesophageal echo) before elective cardioversion. Evidence now supports earlier rhythm control in many patients rather than defaulting to rate control alone.
Catheter ablation
Catheter ablation has become a mainstay of rhythm control. Working in an electrophysiology lab, the operator threads catheters to the left atrium and creates lines of scar that electrically isolate the pulmonary veins — pulmonary vein isolation — cutting off the triggers that start AFib.
For symptomatic paroxysmal AFib, ablation is now considered a reasonable first-line rhythm-control option in suitable patients, and it is more effective than drugs at maintaining sinus rhythm. Energy sources include radiofrequency (heat), cryoablation (cold), and the newer, tissue-selective pulsed-field ablation. Persistent AFib may need more extensive ablation and sometimes a repeat procedure. See the full picture in our cardiac ablation guide.
Lifestyle and risk-factor modification
One of the biggest shifts in modern AFib care is the emphasis on treating the drivers of the arrhythmia, not just the arrhythmia itself. Aggressive risk-factor management can reduce the AFib burden and improve the success of drugs and ablation:
- Weight loss — losing 10% or more of body weight meaningfully reduces AFib episodes in people with obesity.
- Blood-pressure control and management of diabetes.
- Treating obstructive sleep apnea — often dramatically helpful.
- Reducing or stopping alcohol.
- Regular moderate exercise.
These measures are now a formal pillar of guideline-directed AFib care rather than an afterthought.
Key takeaways
- AFib is an irregularly irregular rhythm with no P waves and a fibrillatory baseline.
- It usually starts from pulmonary-vein triggers and is progressive — treating it early matters.
- Its main danger is stroke from clot in the left atrial appendage.
- CHA₂DS₂-VASc guides anticoagulation; DOACs are preferred over warfarin for most.
- Manage the rhythm with rate or rhythm control (drugs, cardioversion, ablation).
- Aggressive risk-factor modification — weight, blood pressure, sleep apnea, alcohol — is now central.
Frequently asked questions
What is atrial fibrillation?
The most common sustained heart-rhythm disorder, in which chaotic electrical activity makes the atria quiver instead of contract, producing an irregularly irregular heartbeat and raising the risk of stroke.
How is atrial fibrillation seen on an ECG?
An irregularly irregular rhythm with no discernible P waves — replaced by a fibrillatory baseline — and usually a narrow QRS.
Why do people with AFib take blood thinners?
AFib lets blood stagnate and clot in the left atrial appendage; anticoagulants prevent a clot from travelling to the brain and causing a stroke. AFib raises stroke risk about fivefold.
What is the CHA₂DS₂-VASc score?
A tool that estimates stroke risk from congestive heart failure, hypertension, age, diabetes, prior stroke, vascular disease, and sex. A score of 2+ in men (3+ in women) generally means anticoagulation is recommended.
Which blood thinner is best for atrial fibrillation?
Direct oral anticoagulants (apixaban, rivaroxaban, dabigatran, edoxaban) are recommended over warfarin for most people because they cause less brain bleeding and need no INR monitoring; warfarin is preferred with mechanical valves or moderate-to-severe mitral stenosis.
What is the difference between rate and rhythm control?
Rate control slows the ventricular response while leaving AFib in place (beta-blockers, calcium channel blockers, digoxin); rhythm control restores normal sinus rhythm with drugs, cardioversion, or ablation.
Can atrial fibrillation be cured?
Catheter ablation (pulmonary vein isolation) can eliminate or greatly reduce AFib, especially paroxysmal AFib, though it sometimes needs repeating; aggressive risk-factor control also lowers the burden.
What lifestyle changes help atrial fibrillation?
Losing excess weight, controlling blood pressure and diabetes, treating sleep apnea, cutting alcohol, and exercising regularly all reduce AFib episodes and improve treatment success.
Is atrial fibrillation dangerous?
It is usually not immediately life-threatening, but untreated it substantially raises the risk of stroke and can lead to heart failure, so it needs proper assessment and treatment.
Sources & further reading
- Cardiovascular Credentialing International (CCI)
- American College of Cardiology
- American Heart Association
- MedlinePlus (U.S. National Library of Medicine)
External links are provided for reference; always confirm current details with the official source.